Visualizing What Needs to Be Done for Better Health
|
Getting to data use: Aggregating and analyzing health data to paint a robust picture of what is working and what needs to be done to improve health outcomes is the purpose of data use. Creating compelling health information products that communicate understanding and lead to action is a key component of data use. These products require time, effort, some technical skill, and a culture of data use, which means that decision makers and service providers want and rely upon quality data as a basis for making decisions about health. Data quality is the fundamental building block, followed by appropriate analysis, and communication of what data mean, in a digestible format that others can understand. Ideally, this kind of presentation of information will influence decision makers and lead them to change or improve health |
For the past year, the USAID-funded MEASURE Evaluation project has been providing technical assistance to a cadre of 14 health professionals in Zambia to create compelling health information products that communicate and lead to action. Following their final session this month (October 2016), the group flew home from Chapel Hill, NC, to Zambia—certificates of achievement tucked into their baggage and a vetted health information communication product stored on their laptops.
The program aimed to work with this select group representing the Zambia Ministry of Health (MOH), the National AIDS Council (NAC), the Ministry of Community Development (MCD), and the University of Zambia (UNZA) to build capacity on analysis of data from national and subnational surveys and from routine data systems in Zambia. Further, the effort required that each participant team analyze data on a chosen topic of national policy and program relevance and present it in a scientific research poster format.
Today and for the next several days, we present profiles of four program participants and their analyses:
Paying it Forward
 Not only does Andrew Banda practice his craft—he teaches it to others. Banda is a lecturer in demography at the University of Zambia in Lusaka. He once was an undergraduate there and then went on to earn post-graduate degrees in population studies at the University of Groningen in The Netherlands and in monitoring and evaluation methods at Stellenbosch University in South Africa.
Not only does Andrew Banda practice his craft—he teaches it to others. Banda is a lecturer in demography at the University of Zambia in Lusaka. He once was an undergraduate there and then went on to earn post-graduate degrees in population studies at the University of Groningen in The Netherlands and in monitoring and evaluation methods at Stellenbosch University in South Africa.
Now he’s back. Teaching, but always learning. “A lot of things will change in the way I do data analysis,” he said during a recent workshop with MEASURE Evaluation, funded by the United States Agency for International Development (USAID) and housed at the Carolina Population Center at the University of North Carolina at Chapel Hill. This workshop was the third of three and was focused on making complex data easy to understand through the use of visuals.
The point of the workshop, Banda said, is that complex data is more likely to be used to improve things if it is easy to understand. For a researcher like himself, that begins with the basics of analyzing the data at hand. “For me, I have improved my research skills in generating an objective, doing the analysis, and presenting the facts. I can teach my students how to propose research, conduct the research, analyze data, and present. I can give them better skills.”
For his workshop data visualization project, Banda and his colleague looked at what determines when children get treatment for illness, specifically the two most common contributors to deaths among children under age five: diarrhea and acute respiratory infections. “In Zambia, most kids come to the health clinic with these symptoms or a fever, but in looking at routine health data, we saw that about 30 percent of children with one of these two symptoms had not been taken to a clinic.”
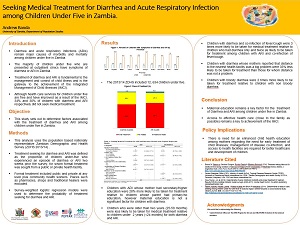 He wondered why. Checking the Zambia Demographic and Health Survey—which is a population survey conducted every five years—he saw the same trend he had spotted in routine health data. The ensuing data triangulation and secondary research he did led to his conclusion that household decisions were the key.
He wondered why. Checking the Zambia Demographic and Health Survey—which is a population survey conducted every five years—he saw the same trend he had spotted in routine health data. The ensuing data triangulation and secondary research he did led to his conclusion that household decisions were the key.
- If a family was far from a clinic, more than the recommended five kilometers, they were less likely to take a sick child to the clinic.
- If the mother had little education, she was less likely to take a child to the clinic.
- If the child was younger than two years, he or she was more likely to be taken to a clinic; but if there was a child younger than the sick one, the family typically paid more attention to the younger child’s health.
- Many families assumed the nearest clinic would not have medicines on hand and so chose to medicate the child with whatever they had at home.
Banda proposed two recommendations based on his research:
- The government should scale up sensitization to mothers that diarrhea or respiratory distress were the two most dangerous health issues for young children so they would more likely decide to visit a clinic for help.
- The government should provide better care and supplies of medicines closer to families. This, of course, would require more money and, therefore, an advocacy campaign aimed at government allocation of resources to increase the number of clinics.
That’s something that, perhaps, Banda’s students will one day tackle.
Analyzing the Causes of Stunted Growth
 The window of most concern for child growth stunting is between the ages of one year and three years. That’s the time period parents, health workers, and the health system as a whole should focus on to solve a big problem in Zambia: as many as 40 percent of children there bear the effects of growth stunting.
The window of most concern for child growth stunting is between the ages of one year and three years. That’s the time period parents, health workers, and the health system as a whole should focus on to solve a big problem in Zambia: as many as 40 percent of children there bear the effects of growth stunting.
Katongo Mumbi is, right now, raising her two children, one of them in that window. She is the research monitoring and evaluation coordinator for the National AIDS Council within the health ministry in Zambia. Recently, she spent several weeks working with MEASURE Evaluation on data analysis, to improve her skills and, specifically for her chosen project, to examine the causes of growth stunting.
Data are part of her daily work life. She studied in England and earned a master’s degree in social sciences. She reviews research done by the health ministry, by large global donors for health projects, and by implementing partners. She’s on the lookout to ensure data quality and to surface anything new in research findings that should be used to adjust health programs and policies.
“I’ve gained a lot of confidence in data analysis in this workshop,” she said, referring to her time with MEASURE Evaluation. “Especially [in using] the STATA statistical software for data analysis and SPSS (an IBM statistical software package for social sciences). It has helped my skills in the interpretation of results.”
Ms. Mumbi began her data analysis project with the available data on child stunting in Zambia relative to HIV exposure. But she went beyond that data and also looked at the age of the mother at childbirth, the birth weight of the child and its gender, and the socio-economic situation of the household, especially access to clean water and adequate sanitation. The latter point is especially important, she says, because lack of clean water can lead to enteropathy, an inflammation of the digestive system that leads to nutrients not being absorbed.
 Her question of the data: is there something underlying that could overcome the stunting among children; and, if you catch the stunting early, can it be reversed? In other words: what can Zambia learn to do better by its children?
Her question of the data: is there something underlying that could overcome the stunting among children; and, if you catch the stunting early, can it be reversed? In other words: what can Zambia learn to do better by its children?
Her analysis revealed that exposure to HIV is not the determining factor and that the health system needs to probe further into the causes of growth stunting. “The focus should be between the ages of one and three years,” she said. “Many children in this age group in urban settings go to play school and are not the focus of family attention.” She reflected on her own situation. She leaves her two children, both under age five, with a relative while she works. “I leave them good food—yogurt and fruit, for example—but what if those good choices aren’t given?”
The upshot of her analysis is that she needs to work to generate interest within the health ministry to probe more deeply into the causes of child stunting. “Maybe we focus too much on HIV status, but what about thereafter?” she wonders. She is passionate about the quest for answers. “Stunting leads to lower cognitive development, school dropout, and lower incomes,” she says. She hopes to make a difference, as stunting lasts a lifetime and has important consequences for families and for the country.
Promoting Deliveries with Skilled Birth Attendants
 Trust Mfune, works in monitoring and evaluation (M&E) for the Zambian health ministry. His training is in economics. He lives in Lusaka, and is father to two boys and a girl. It’s telling that he gives their ages in terms of their grade in school—fourth grade, second grade, and kindergarten. Maybe that’s because his wife is a teacher.
Trust Mfune, works in monitoring and evaluation (M&E) for the Zambian health ministry. His training is in economics. He lives in Lusaka, and is father to two boys and a girl. It’s telling that he gives their ages in terms of their grade in school—fourth grade, second grade, and kindergarten. Maybe that’s because his wife is a teacher.
His data analysis project concerns antenatal care (ANC) and skilled birth assistance. It piqued his curiosity why ANC rates in Zambia are high and going up, but the number of women choosing to give birth in a facility where skilled birth attendants are available is low.
It’s recommended that women have four antenatal visits during their pregnancies. Most women make at least the first clinic visit, but visits fall off thereafter. “We were focused on the coverage,” he says.
It’s better for the woman and the infant to have births attended by a skilled birth attendant, he says. “The woman can be checked thoroughly and the baby checked. And in the facility, the equipment is there [if there is a problem], providing better survival for mother and baby.”
As he investigated why “high” ANC coverage did not lead to greater numbers of births in facilities, he discovered the data were showing “coverage” as even one visit, thus showing a high rate when, in fact, ANC visits fell off sharply after the first visit.
The data also told him that geography was a factor in rural areas, because women were less likely to give birth in a facility if it was far from home. And a key factor was the woman’s education level. The longer she attended school, the more likely she was to understand the value in having the full complement of four antenatal care visits.
From these data, he and his team devised three main recommendations:
- The country should focus on increasing the number of ANC visits (more than one visit) in order to increase the number of institutional deliveries
- In rural areas, the government should increase the number of health facilities to reduce distances women have to travel for ANC visits and attended births—also, if families have transport, they are twice as likely to choose delivery in a health facility
- The MOH and the Ministry of Education should work together to encourage education for girl children and also to get very young mothers back into school
He knows that this will take a concerted effort by the government and feels confident that the government is committed to adding health clinics in rural areas. The effort to keep girls in school will mean a change in the typical cut-off point for girls’ education to keep them in school longer. This also, he says, will require an education campaign aimed at parents to help them understand the benefits of keeping their daughters in school rather than taking them out to work at home.
In about two to three years, Mfune plans to revisit his data and what actions have been taken regarding his recommendations.
Education Should Help Women Choose Modern Contraceptives
 Boyd Kaliki is a provincial monitoring and evaluation (M&E) officer with the MOH in Lusaka, Zambia, the nation’s capital. He supports and monitors the country’s agreement with the Centers for Disease Control and Prevention (CDC), focusing on programs to prevent HIV transmission—such as voluntary male medical circumcision and prevention of mother-to-child transmission—and enrollment in HIV treatment and care.
Boyd Kaliki is a provincial monitoring and evaluation (M&E) officer with the MOH in Lusaka, Zambia, the nation’s capital. He supports and monitors the country’s agreement with the Centers for Disease Control and Prevention (CDC), focusing on programs to prevent HIV transmission—such as voluntary male medical circumcision and prevention of mother-to-child transmission—and enrollment in HIV treatment and care.
Kaliki is on daily speaking terms with DHIS 2, the health data software platform used throughout Zambia and in many other low- and middle-income countries. And so, he knows the power of this software platform to generate visuals that convey the story that health data can tell. He’s also a formally educated statistician. For this training, he chose to focus on merging data sets, because he noticed from the data that many HIV-positive women of childbearing age were not using modern contraceptives. He wondered why.
First, some background: the data show that in Zambia only 33 percent of all women of childbearing age are using modern contraceptives. Interestingly, that figure is higher—37 percent—among HIV-positive women of childbearing age. “So maybe they know the dangers of getting pregnant,” he says. But, given those dangers, the figure isn’t high enough, he reasoned, given the compromised immunity of these women. Also, there is the added issue of potential HIV transmission to their infants.
To learn more, he compared the data set of all females with HIV-positive women—those who use contraceptives and those who don’t. He merged that set with other data sets: level of education, number who are married, age, and the number who intend to become pregnant. When compared, he found these combined data sets provided additional insight:
- The more education an HIV-positive woman attains, the higher the likelihood that she will use contraceptives.
- The age of the woman increases the likelihood she will use contraceptives—a 2 percent increase for every one year of age attained.
- Those women living in rural settings are 26 percent less likely to use contraceptives than their urban counterparts, which is likely a factor of distance to clinics where contraceptives are available.
Kaliki knows that the Ministry of Health would like to see more HIV-positive women taking charge of their childbearing—to safeguard their health and to reduce HIV transmission to their children. Lower transmission of HIV could help the country reduce its overall HIV rate of 13.3 percent. “Too high,” he says.
Using his combined data sets, Kaliki proposes three recommendations for action:
- The government should integrate HIV testing, counseling, and treatment programs with family planning programs.
- The government should expand and improve health education so that HIV-positive women understand how pregnancy affects their immune system and so they know ways to protect their health, both when they are not pregnant and when they are.
- The government should strengthen incentives for families to keep their girls in school as well as incentives for use of modern family planning methods. “There already are policies,” he said, “and reinforcing those is the way to go.”
For more information, visit www.measureevaluation.org.











